
The Mosquito-Borne Diseases Discussed in This Guide:
West Nile virus (WNV) — the #1 mosquito-borne disease threat in the U.S.; over 63,000 cases reported between 1999 and 2025
Mosquito-borne encephalitis — including La Crosse (LAC), Eastern equine (EEE), and Jamestown Canyon virus (JCV)
Chikungunya — reached the Americas in 2006 via travelers; local U.S. cases reported in Florida (2014 & 2025), Texas (2015), New York (2025)
Dengue — globally, an estimated 390 million infections annually; local U.S. cases in Florida, Hawaii, and the Texas-Mexico border
Malaria — eliminated from the U.S. after 1950, but the primary vector mosquito (Anopheles quadrimaculatus) is still abundant in the southeastern U.S.
Heartworm — reported in all 50 U.S. states; primarily affects dogs
Quick Facts
Globally, up to a million people die each year from mosquito-borne diseases. In the U.S., West Nile virus remains the leading threat — the deadliest year on record was 2012, with 286 deaths reported to the CDC. The largest outbreak was in 2003, with 9,862 cases and 264 deaths.
How Many People Die from Mosquito-Borne Diseases?
Mosquitoes are responsible for some of the world’s most deadly diseases. It is estimated that up to a million people die every year from mosquito-borne diseases globally, with many countries ravaged by malaria, yellow fever, and dengue-hemorrhagic fever.
In the United States, West Nile virus is the leading mosquito-borne killer. The deadliest year on record was 2012, when 286 deaths were reported to the CDC. The largest single-year outbreak occurred in 2003, with 9,862 reported cases and 264 deaths. Between 1999 and 2016, over 46,000 WNV cases were reported in the U.S. For year-by-year case data and current trends, see VDCI’s 2025 Mosquito-Borne Disease Year in Review.
Common Mosquito-Borne Diseases in the United States
There are really only two reasons to control mosquitoes; to avoid nuisance biting and to control mosquito-transmitted diseases in the USA. Everyone recognizes that mosquitoes can be a terrible blood feeding nuisance, but many people do not realize the magnitude of the health threat that they represent globally. Some of the world’s most deadly diseases are carried and transmitted by mosquitoes. It is estimated that up to a million people die every year from mosquito-borne diseases with many countries around the world ravaged by malaria, yellow fever, and dengue-hemorrhagic fever. What is the history and what are the current local cases of mosquito-borne diseases in the U.S.?
Malaria in the U.S.: A History (and Why It Still Matters)
Malaria is one of the most dangerous mosquito transmitted diseases caused by a Plasmodium parasite and is the leading cause of mosquito-borne deaths throughout the world. In the past, local malaria cases were reported within the U.S. It wasn’t until after 1950 that malaria was considered eliminated from the country, due to large-scale mosquito control efforts and swamp drainage. While the disease is not currently a threat, one of the primary carriers of the disease parasite in the pre-1950s U.S. – is far from eliminated. Anopheles quadrimaculatus (also known as the Common Malaria Mosquito) is distributed throughout the eastern United States, often occurring in huge numbers in the southeastern states, especially along the Gulf of Mexico. This fact reinforces the importance of robust surveillance and disease testing programs highlighting the potential resurgence of mosquito diseases in areas where the species inhabits.

What Diseases Do Mosquitoes Carry in the USA?
In more recent years, West Nile virus, several types of encephalitis, and dog heartworm have been the primary mosquito-borne diseases in the U.S. Additionally, Zika virus, dengue fever, and chikungunya have emerged over the past couple of years as threats to human health in the United States, South America, and the Caribbean. These mosquito transmitted diseases represent a significant public health challenge.
What is Mosquito-Borne Encephalitis?
Mosquito-borne encephalitis is one of the critical mosquito transmitted diseases that can severely impact human health. Mosquito-borne encephalitis can be a severe result of many viruses vectored by mosquitoes. In the U.S., it is geographically wide-spread and is prevalent in several forms: West Nile virus (WNV), La Crosse encephalitis (LAC), eastern equine encephalitis (EEE), Jamestown Canyon virus (JCV), and several others. Encephalitis is an inflammation of the brain and central nervous system and is characterized by a high to moderate mortality rate, with some survivors left with permanent physical and mental disabilities.
West Nile Virus: #1 Mosquito-Borne Disease Threat in the U.S.
West Nile virus, one of the leading mosquito-borne diseases in the USA, can cause encephalitis in severe cases. This mosquito disease entered the U.S. along the east coast in 1999 and has had serious ongoing implications for the rest of North America as it has spread across the country. 47 out of 50 states and the District of Columbia reported West Nile virus infections in people, birds, or mosquitoes in 2017.
WNV is typically transmitted to humans by mosquitoes that have previously fed upon an infected bird. While over 150 species of mosquitoes have been known to carry WNV, the primary vector species in the U.S. are Culex pipiens, Culex tarsalis, and Culex quinquefasciatus. These mosquitoes are all active at night, and most cases of infection occur during the summer months. Approximately 20% of people affected by WNV will experience flu-like symptoms including fever, headache, nausea, muscle pain, and swollen lymph glands. Other symptoms may include a stiff neck, rash, sleepiness or disorientation. In severe cases, an individual can develop West Nile Encephalitis or Meningitis, which can lead to coma, tremors, convulsions, paralysis, and even death.
2003 was the largest WNV outbreak in the U.S. with 9,862 cases reported and 264 deaths. 2012 was the deadliest year for WNV in the U.S., with 286 deaths reported to the CDC. West Nile virus remains the #1 mosquito-borne disease threat to humans in the U.S. Approximately 2,000 cases are reported each year, though the true number is likely much higher since most infections produce no symptoms or only mild flu-like illness. For year-by-year case data and emerging trends, see our 2025 Mosquito-Borne Disease Year in Review.
Chikungunya Virus in the U.S.: Local Cases in Florida and Texas
WNV, EEE, LAC, and a few other mosquito-borne encephalitis viruses have an animal reservoir and cannot be transmitted from human to mosquito. Mosquito-transmitted diseases like Chikungunya is another illness that primarily affects humans. Mosquitoes become infected when they feed on a person already infected with the virus and then spread the virus by feeding on other humans. Because of this ability, the virus has the potential to spread quickly, especially in urban areas with larger populations. The virus first reached the Americas in 2013, with local cases reported in the U.S. in Florida (2014) and Texas (2015).
Dengue Virus: A Growing Threat in U.S. Urban Areas
Dengue virus, another human virus, is transmitted by certain Aedes mosquitoes. On a global level, the virus is considered a significant threat as our world’s urban landscapes grow. Beyond the increase in desirable habitats for the container-breeding species, the virus has four strains (multiple serotypes). These mosquito diseases thrive in urban environments, making it complicated for medical professionals to manage. Chikungunya virus shares similar symptoms to dengue and provides those bitten with immunity from future chikungunya infections. Unfortunately, with multiple strains of dengue, an individual is more likely to be hospitalized or die if infected with more than one serotype. Dengue is considered under reported or misclassified. The World Health Organization posted an update on the virus globally, citing research1 that estimates the real number of dengue infections could be close to 390 million annually.
The United States has experienced local cases of dengue in Florida, Hawaii, and near the Texas-Mexico border. Larger outbreaks have occurred within U.S. Territories, including Puerto Rico, the U.S. Virgin Islands, and U.S.-affiliated Pacific Islands.
Heartworm Disease in Dogs: A Mosquito-Borne Threat to Pets

In addition to human cases of mosquito-borne diseases, there is a growing concern for pet owners. Dirofilaria immitis, commonly referred to as heartworm, is a parasitic roundworm that infects a variety of mammals. Heartworm is found throughout the world and has been reported in all states in the U.S. The natural host is dogs. Infection in dogs can lead to heartworm disease and, if left untreated, severe physical damage and death may occur. Fortunately, for felines, most worms in cats don’t survive to the adult stage. Prevention is an option, for both dogs and cats, and should be discussed with your veterinarian. Although isolated human infections have been reported, heartworm is not currently recognized as a human health problem. Mosquito-borne diseases like Heartworm have been reported in all U.S. states.
Which Mosquitoes Are Most Dangerous in the U.S.?
Of the roughly 200 mosquito species found in the United States, only about a dozen pose a meaningful disease risk. The most concerning species are:
- Culex pipiens, Culex tarsalis, and Culex quinquefasciatus — the primary vectors of West Nile virus across North America. Active at night, breeds in stagnant water.
- Aedes aegypti (the yellow fever mosquito) — feeds exclusively on human blood and is the primary vector for Zika, dengue, chikungunya, and yellow fever. Found across the southern U.S.
- Aedes albopictus (the Asian tiger mosquito) — an aggressive daytime biter and secondary vector for several arboviruses; range expanding northward with climate change.
- Anopheles quadrimaculatus — the historic U.S. malaria vector. Still abundant in the southeastern U.S., which is why surveillance remains important even though malaria was eliminated domestically in 1950.
- Culiseta melanura — the primary EEE vector in coastal swamps.
For a deeper look at these species, see our guide to the 5 mosquitoes of public health concern in the United States.
Why Mosquito Control Matters for Public Health
As an individual, if you’ve ever been driven inside by biting mosquitoes or have chased the pesky invaders around the bedroom in the middle of the night, you may consider 1 or 2 mosquitoes – too many. When mosquito populations increase, mosquito diseases pose even greater risks and , there becomes an even greater need for control efforts. Hurricanes have the ability to create vast areas of standing water that produce extreme mosquito populations and make the already difficult disaster relief efforts even harder and more dangerous. With or without a natural disaster, economic losses can be considerable for businesses or travel destinations that are considered uninhabitable or unsuitable. This is often due to unmanaged environments that allow for large populations of one of nature’s deadliest – the mosquito. The impact mosquito-transmitted diseases in the USA can have on our communities goes beyond itchy bites. We must continue to manage abundant mosquito populations to help protect public health from mosquito-borne diseases. Effective protection starts with an Integrated Mosquito Management program that combines surveillance, larval and adult control, and disease testing — and in emergency situations following hurricanes or floods, aerial application can rapidly reduce populations across large areas.
1 Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL et.al. The global distribution and burden of dengue. Nature;496:504-507.
Frequently Asked Questions About Mosquito-Borne Diseases
What diseases do mosquitoes carry in the U.S.?
The most common mosquito-borne diseases in the United States are West Nile virus, Eastern equine encephalitis, La Crosse encephalitis, Jamestown Canyon virus, St. Louis encephalitis, dengue, chikungunya, and heartworm (which affects dogs). West Nile virus is by far the most frequently reported.
How many people die from mosquitoes each year?
Globally, mosquitoes kill an estimated 725,000 to 1 million people each year, primarily from malaria. In the United States, mosquito-borne disease deaths typically range from 100 to 300 annually, with West Nile virus being the leading cause.
What is the most dangerous mosquito-borne disease in the U.S.?
West Nile virus is the most common, but Eastern equine encephalitis (EEE) is the deadliest, with a mortality rate of roughly 33% among those who develop severe symptoms.
Are there mosquitoes in the United States?
Yes — approximately 200 mosquito species are found in the U.S., though only about a dozen are known to transmit diseases to humans.
How can I protect my community from mosquito-borne diseases?
The most effective approach is an Integrated Mosquito Management (IMM) program that combines surveillance, larval control, adult mosquito control, and public education. Personal protection includes following the “4 Ds”: Defend (use EPA-approved repellent), Dress (wear long sleeves and pants), Drain (eliminate standing water), and Dusk & Dawn (limit outdoor activity when mosquitoes are most active).
Contact Us to Learn More About Effective Mosquito Prevention Strategies:
![]() Since 1992, Vector Disease Control International (VDCI) has taken pride in providing municipalities, mosquito abatement districts, industrial sites, planned communities, homeowners associations, and golf courses with the tools they need to run effective mosquito control programs. We are determined to protect the public health of the communities in which we operate. Our mosquito control professionals have over 100 years of combined experience in the field of public health, specifically vector disease control. We strive to provide the most effective and scientifically sound mosquito surveillance and control programs possible based on an Integrated Mosquito Management approach recommended by the American Mosquito Control Association (AMCA) and Centers for Disease Control and Prevention (CDC). VDCI is the only company in the country that can manage all aspects of an integrated mosquito management program, from surveillance to disease testing to aerial application in emergency situations.
Since 1992, Vector Disease Control International (VDCI) has taken pride in providing municipalities, mosquito abatement districts, industrial sites, planned communities, homeowners associations, and golf courses with the tools they need to run effective mosquito control programs. We are determined to protect the public health of the communities in which we operate. Our mosquito control professionals have over 100 years of combined experience in the field of public health, specifically vector disease control. We strive to provide the most effective and scientifically sound mosquito surveillance and control programs possible based on an Integrated Mosquito Management approach recommended by the American Mosquito Control Association (AMCA) and Centers for Disease Control and Prevention (CDC). VDCI is the only company in the country that can manage all aspects of an integrated mosquito management program, from surveillance to disease testing to aerial application in emergency situations.











 The species has been the focus of much industry news this year because of its ability to transmit
The species has been the focus of much industry news this year because of its ability to transmit 

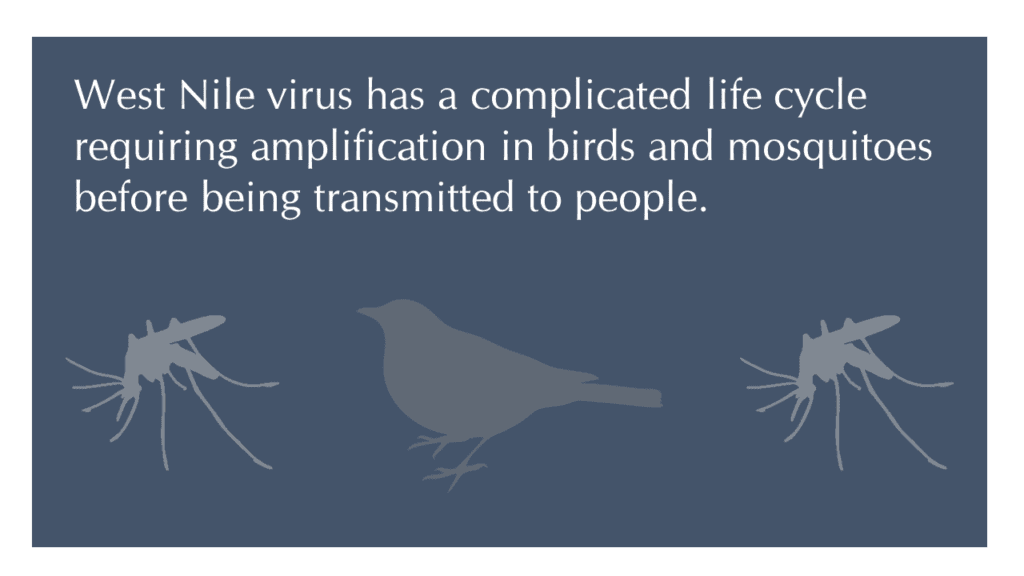

 When a new disease enters an area, disease ecologists expect to see major die-offs in the first year. However, over time, the impact of the disease is expected to decrease as the host population experiences increased immunity and can recover. Using data collected from over a quarter of a million birds belonging to 49 species, researchers have found that about half of the avian species affected by West Nile virus have made a recovery; however, the other half are continuing to experience major decreases in their population. Given the additional pressures on bird populations throughout the United States, of climate change, altered land use patterns, and feral cats, the added impact of West Nile on these populations is concerning.
When a new disease enters an area, disease ecologists expect to see major die-offs in the first year. However, over time, the impact of the disease is expected to decrease as the host population experiences increased immunity and can recover. Using data collected from over a quarter of a million birds belonging to 49 species, researchers have found that about half of the avian species affected by West Nile virus have made a recovery; however, the other half are continuing to experience major decreases in their population. Given the additional pressures on bird populations throughout the United States, of climate change, altered land use patterns, and feral cats, the added impact of West Nile on these populations is concerning.
 The city of Jonesboro, Arkansas is already preparing for the 2016 mosquito season. The city’s sponsored public affairs program “Let’s Talk, Jonesboro!” featured Jim Stark, a member of the Vector Disease Control International (VDCI) team, to provide details.
The city of Jonesboro, Arkansas is already preparing for the 2016 mosquito season. The city’s sponsored public affairs program “Let’s Talk, Jonesboro!” featured Jim Stark, a member of the Vector Disease Control International (VDCI) team, to provide details. Jim spoke with host Roy Ockert Jr. about Zika virus, the importance of knowing the
Jim spoke with host Roy Ockert Jr. about Zika virus, the importance of knowing the 
 Ae. aegypti, the yellow fever mosquito, is a medium-sized mosquito easily distinguished from Ae. albopictus by a silvery-white “lyre-shaped” pattern of scales on its scutum. Both species are peridomestic species found not far from human dwellings, and are particularly abundant in towns and cities. They are primarily early morning or late afternoon feeders, but females can also take a blood meal at night under artificial illumination. Aedes aegypti is reported to fly only a few hundred yards from breeding sites. Larvae can be found in a variety of
Ae. aegypti, the yellow fever mosquito, is a medium-sized mosquito easily distinguished from Ae. albopictus by a silvery-white “lyre-shaped” pattern of scales on its scutum. Both species are peridomestic species found not far from human dwellings, and are particularly abundant in towns and cities. They are primarily early morning or late afternoon feeders, but females can also take a blood meal at night under artificial illumination. Aedes aegypti is reported to fly only a few hundred yards from breeding sites. Larvae can be found in a variety of 



 The Zika virus was first isolated from a rhesus macaque in Uganda in 1947 and documented in humans as early as 1968. The reason we haven’t heard much about Zika until now is that the vast majority of human cases present with little to no symptoms. In fact, the CDC reports that only 1 in 5 individuals who contract the virus will become ill, and those that do will experience mild flu-like symptoms including fever, rash, joint pain, headache and conjunctivitis (red eyes).
The Zika virus was first isolated from a rhesus macaque in Uganda in 1947 and documented in humans as early as 1968. The reason we haven’t heard much about Zika until now is that the vast majority of human cases present with little to no symptoms. In fact, the CDC reports that only 1 in 5 individuals who contract the virus will become ill, and those that do will experience mild flu-like symptoms including fever, rash, joint pain, headache and conjunctivitis (red eyes). Zika is spread to humans by the Aedes genus of mosquito. The most common vectors for transmitting Zika include Aedes aegypti (Yellow Fever mosquito) and
Zika is spread to humans by the Aedes genus of mosquito. The most common vectors for transmitting Zika include Aedes aegypti (Yellow Fever mosquito) and 